From Distress to Agency: Self-Language Change and Self-Care Activation in AI-Guided Therapeutic Conversation
Abstract
Importance. Digital therapeutic platforms can widen access to mental-health support by making evidence-informed self-care tools available at the moment a person is ready to use them. For AI-guided therapeutic conversation, a central scientific question is whether real sessions help users translate distress, uncertainty, and emotional disclosure into language of agency, action, insight, relief, and self-care.
Objective. To evaluate whether AI-guided therapeutic conversation in Habit of Living was associated with measurable shifts in user self-language, journal language, progress tracking, cognitive reframing, structured self-care activity, clinical assessment movement, and safety signals.
Design. Retrospective observational study of de-identified Habit of Living platform records through June 20, 2026. The primary evidence streams were saved AI-guided therapeutic conversation sessions, journal entries, progress tracking, cognitive-reframing records, and structured self-care activity. Standardized mental-health and wellbeing assessments were analyzed as external clinical triangulation because repeated assessment coverage was smaller than the content-centered data streams.
Exposure. First saved AI-guided therapeutic conversation and subsequent saved conversation sessions. Content analyses used aggregate markers in user-written conversation and journal text; raw text was excluded from manuscript tables and figures.
Main outcomes. Within-session change in user-language markers from the first to last third of a session; cross-session marker change among repeat users; journal-language change in the 90 days before versus after first conversation; progress-tracker change in the 30 days before versus after first conversation; cognitive-reframing change in the 90 days before versus after first conversation; structured self-care activation; repeated-assessment clinical triangulation; and aggregate safety monitoring.
Results. The study included 16,487 users with saved AI-guided conversation exposure, 31,564 saved sessions, and 229,562 saved exchange records from April 11, 2023 to June 20, 2026. In 25,310 analyzable saved sessions from 13,501 users, user language shifted by session end toward agency (+15.1 pp), relief/hope (+14.1 pp), action planning (+3.1 pp), and insight/meaning (+3.0 pp), while distress decreased modestly (-1.5 pp). Among 5,615 users with paired journal windows, post-conversation journaling was more frequent and showed lower distress (-1.6 pp) and uncertainty/stuckness (-4.4 pp), while other journal-language markers moved in mixed directions. Structured self-care activity increased across multiple therapeutic tool areas, Happiness improved by +4.92 points among 6,179 paired users, and cognitive-reframing records showed greater positive-reframe completion (+10.2 pp) and more agency-oriented positive reframes (+4.9 pp). Repeated-assessment triangulation was directionally favorable (26.5% material improvement in exposed intervals versus 20.6% in comparison intervals) and statistically imprecise (0.07 SD (-0.16 to 0.30), p=0.533).
Interpretation. The clearest signal was a content-and-activation pattern: users' own language shifted within sessions toward agency, action planning, insight, and relief; cognitive reframing and structured self-care activity increased; and Happiness tracking improved descriptively. Journal writing became more frequent and less marked by distress and stuckness, although other journal-language markers moved in mixed directions. These findings support a self-language activation model for mental-health AI, in which AI-guided therapeutic conversation may help users organize distress into insight, agency, and structured self-care behavior. Clinical effectiveness, marker validity, and safety require prospective controlled evaluation with validated endpoints, human-coded language validation, and adjudicated safety review.
Key Points
- In 25,310 analyzable saved sessions from 13,501 users, the user's own language shifted toward agency (+15.1 pp), relief/hope (+14.1 pp), action planning (+3.1 pp), and insight/meaning (+3.0 pp) from the first to last third of sessions.
- In journal entries from 5,615 users, post-conversation writing was more frequent and showed less distress (-1.6 pp) and less uncertainty/stuckness (-4.4 pp); other journal-language markers moved in mixed directions.
- Happiness tracking improved by +4.92 points among 6,179 paired users, and cognitive reframing showed higher positive-reframe completion (+10.2 pp) and fewer cognitive distortions flagged (1.43 fewer).
- Repeated standardized assessments provided supportive clinical triangulation, with higher material improvement in conversation-exposed intervals (26.5% versus 20.6%) and an imprecise adjusted association (0.07 SD (-0.16 to 0.30)).
Introduction
Access is one of the central problems in mental health. Many people face cost, availability, stigma, geography, timing, or continuity barriers that limit their ability to receive therapeutic support when they need it. Habit of Living was built to expand access to therapeutic tools through a digital format, giving users agency to act in favor of their mental wellbeing with tools that are often available only inside scheduled therapy sessions or other high-barrier care settings.
AI-guided therapeutic conversation is important in this context because conversation can be the moment when a person names distress, organizes a difficult experience, receives reflective support, and chooses a next step. The impact of such a system should be visible inside the language of the session itself and in adjacent self-care behavior: journal writing, progress tracking, cognitive reframing, structured therapeutic exercises, and safety signals.
Prior reviews of mental-health conversational agents report promising but heterogeneous effects, with stronger evidence for some depression and distress outcomes than for global wellbeing, anxiety, stress, or longer-term functioning [9-11]. Large language model applications in mental health remain early and safety-sensitive [10]. This study extends that literature by evaluating a real-world AI-guided therapeutic conversation system embedded within a broader self-care platform and by making conversation content the primary analytic object.
The central thesis is that AI-guided therapeutic conversation may create value by helping users convert distress and uncertainty into self-language of agency, insight, action, relief, and self-care. The study therefore tests a self-language activation model: a content-centered account of how therapeutic conversation may organize emotional distress into language and behavior that support self-care. Standardized assessments remain important. Repeated assessment uptake was much smaller than the available conversation, journal, and progress-tracking data, so assessments are treated here as external clinical triangulation.
Methods
Study Design and Setting
This was a retrospective observational study of de-identified Habit of Living platform records. Habit of Living is a digital mental-health and self-care platform designed to expand access to therapeutic tools, including AI-guided therapeutic conversation, journaling, emotional regulation, goal setting, trauma processing, exposure practice, relationship reflection, cognitive reframing, recovery support, sleep reflection, habit work, visualization, and progress tracking.
The study was designed to measure content change and self-care activation at the level of the individual user. Causal clinical efficacy remains a prospective research question because users chose when and how to engage with conversation, journaling, trackers, assessments, and self-care activities.
Evidence Streams
Table 1. Evidence streams and analytic role.
| Evidence stream | Scope | Analytic role |
|---|---|---|
| Therapeutic conversation content | 25,310 analyzable saved sessions from 13,501 users | Primary evidence stream for within-session shifts in the user's own language. |
| Longitudinal conversation content | 1,635 repeat-session users | Tests whether language patterns differ between earlier and later saved sessions for the same person. |
| Journal language | 5,615 users with journal entries before and after first saved conversation | Assesses whether language in reflective writing changes around first AI-guided conversation use. |
| Progress tracking | 6,183 users with paired tracker data | Measures near-term self-reported movement in tracked wellbeing domains. |
| Cognitive reframing | 484 users with reframing records before and after first saved conversation | Assesses movement in a structured cognitive-reframing tool connected to therapeutic work. |
| Structured self-care activity | 15,970 users with paired activity records | Measures whether users moved from conversation into therapeutic exercises and self-care tools. |
| Clinical assessment triangulation | 413 repeated-assessment intervals from 74 users | Provides external clinical context while recognizing that assessment uptake was optional and newer than the core conversation, journal, and tracker surfaces. |
| Safety monitoring | 407 PHQ-9 item 9 attempts plus conversation safety markers | Keeps risk signals visible alongside benefit and activation signals. |
Operational Definitions
Table 2. Operational definitions.
| Term | Definition |
|---|---|
| Saved conversation exchange record | A saved unit of AI-guided therapeutic conversation containing a user message, an AI response, or both. Records measure conversation exposure and content; sessions are assembled from related saved records. |
| AI-guided therapeutic conversation session | A saved conversation episode with the AI-guided therapeutic system. Sessions vary in length, so analyses report both users and sessions. |
| User-language marker | A reproducible aggregate text marker in user-written content, such as distress, uncertainty, emotional disclosure, agency, action planning, insight, relief, or self-compassion language. |
| Journal-language window | The user's journal entries in the 90 days before and 90 days after first saved AI-guided conversation. |
| Progress tracking window | The user's tracked progress records in the 30 days before and 30 days after first saved AI-guided conversation. |
| Cognitive-reframing window | The user's cognitive-reframing records in the 90 days before and 90 days after first saved AI-guided conversation. |
| Clinical assessment triangulation | A supporting analysis of repeated standardized mental-health or wellbeing assessments 7 to 180 days apart. This stream is clinically informative and smaller than the content-centered streams. |
| Safety signal | An aggregate monitoring measure such as crisis-language markers, AI safety-resource markers, PHQ-9 item 9 positivity, or assessment worsening. These are screening signals and require adjudication for clinical safety conclusions. |
Marker Denominators and Weighting
Because language markers carry the main contribution of this study, denominator clarity is central. Marker percentages are rates of analyzable text units containing the relevant marker. They are not word shares, symptom scores, diagnoses, or clinician ratings.
Table 3. Marker denominators and weighting.
| Analysis stream | Unit of analysis | Numerator | Denominator | Weighting | Text source |
|---|---|---|---|---|---|
| Within-session conversation language | Session third | User-message records in the session third containing a marker | Analyzable user-message records in that session third | Session thirds are averaged within user, then users are averaged equally | User-written conversation text only |
| Cross-session conversation language | Saved session | User-message records in earlier or later sessions containing a marker | Analyzable user-message records in earlier or later sessions | Session marker rates are averaged within user segment, then users are averaged equally | User-written conversation text only |
| Journal language | Journal entry in a user-window | Journal entries in the 90-day user-window containing a marker | Analyzable journal entries in that same 90-day user-window | Entry rates are averaged within user-period, then users are averaged equally | User-written journal text only |
| Cognitive reframing | Cognitive-reframing record | Records with a completed positive reframe or marker in the relevant thought field | Analyzable cognitive-reframing records in the 90-day user-window | Record rates are averaged within user-period, then users are averaged equally | User-entered negative thoughts and positive reframes |
| Topic and AI-technique markers | Saved exchange record | Saved records whose user text or AI response contains the marker | Saved exchange records with analyzable text for the relevant speaker | Record-weighted descriptive rates | User text for topics; AI response text for technique markers |
| Safety markers | Text field | User-text fields with crisis-language markers or AI-response fields with safety-resource markers | Analyzable fields for the relevant speaker | Field-weighted screening rates | User text for crisis markers; AI response text for safety-resource markers |
Marker Codebook and Validation Status
The marker system used deterministic text patterns selected to capture broad therapeutic-process constructs. The current study uses those markers as reproducible aggregate process measures. Human validation is required before treating marker presence as a validated measure of therapeutic quality.
Table 4. Marker construct codebook.
| Marker | Construct captured |
|---|---|
| Distress | Anxiety, sadness, hopelessness, shame, guilt, trauma, panic, overwhelm, stress, fear, anger, or isolation language. |
| Uncertainty / stuckness | Language such as not knowing what to do, feeling confused, feeling stuck, or being unable to understand a problem. |
| Emotional disclosure | First-person feeling statements and direct emotional expression. |
| Agency | First-person capacity, intention, choice, need, effort, commitment, or ability language. |
| Action planning | Next steps, practice, scheduling, trying, starting, asking, calling, walking, journaling, breathing, or other concrete action language. |
| Insight / meaning | Realization, understanding, noticing, awareness, learning, pattern recognition, or explanatory meaning language. |
| Relief / hope | Feeling better, calmer, relieved, hopeful, proud, grateful, helped, lighter, safe, or thankful. |
| Self-compassion | Kindness toward self, forgiveness, self-compassion, deservedness, trying, or doing one's best. |
Table 5. Marker validation status.
| Validation element | Current status | Publication implication |
|---|---|---|
| Dictionary and codebook | Implemented as deterministic aggregate marker patterns and summarized in this manuscript. | Supports reproducibility, while detailed pattern review should remain available in analytic code. |
| User-only text confirmation | Implemented for primary conversation and journal analyses. | Protects primary claims from AI-response wording and UI-copy contamination. |
| Prompt/template exclusion | Primary analyses use stored user text fields and journal text fields, not prompt templates or page labels. | Supports content validity for user-language claims. |
| Blinded human-coded sample | Not yet completed in the current aggregate study. | Required before strong claims about therapeutic quality or construct-level marker accuracy. |
| Interrater reliability and precision/recall | Not yet completed in the current aggregate study. | Required for top-tier publication claims that depend on automated marker validity. |
Analytic Windows
The primary content analysis compared the first and last thirds of saved conversation sessions. This design measures whether a session ended with a different kind of user self-language than it began with. Longitudinal analyses then examined repeat sessions, journal entries, progress tracking, cognitive reframing, and structured self-care activity around first saved AI-guided conversation.
Table 6. Analytic windows.
| Analysis | Comparison | Interpretation |
|---|---|---|
| Within-session conversation language | First third versus last third of each saved session | Primary test of whether a session moves user language from distress and disclosure toward agency, action, insight, and relief. |
| Cross-session conversation language | Earlier saved sessions versus later saved sessions among repeat users | Tests whether later conversation episodes show durable changes in the language users bring into therapy. |
| Journal language | 90 days before versus 90 days after first saved conversation | Tests whether reflective writing around the same user becomes less distressed or stuck after conversation begins. |
| Progress tracking | 30 days before versus 30 days after first saved conversation | Describes same-person movement in tracked wellbeing categories. |
| Cognitive reframing | 90 days before versus 90 days after first saved conversation | Measures whether structured reframing records become more complete and agency-oriented. |
| Structured self-care activity | 30 days before versus 30 days after first saved conversation | Measures activation into therapeutic tools after conversation starts. |
| Clinical assessment triangulation | Assessment intervals with versus without AI-guided conversation exposure | Provides supporting clinical context with adjusted and sensitivity models. |
Text Marker Analysis
Conversation and journal text were reduced to aggregate markers before reporting. The marker set covered distress, uncertainty or stuckness, emotional disclosure, agency, action planning, insight or meaning, relief or hope, and self-compassion. The primary language claims are based on user-written text. AI-response technique markers were analyzed separately to describe the content of the AI-guided experience and to support artifact checks.
These markers are process measures. They should be read as reproducible indicators of language movement and as a basis for human-rater validation. They are not diagnoses or definitive measures of therapeutic quality.
Statistical Analysis
Within-person marker changes were summarized as mean percentage-point differences with approximate 95% confidence intervals. In the within-session analysis, sessions required at least three analyzable user-message records; marker rates were computed for the first and last thirds of each session, averaged across sessions within user, and then averaged across users. In journal analyses, entry-level marker rates were averaged within the pre and post windows for each user, then averaged across users. Progress trackers were directionally coded so favorable movement is positive. For Anxiety, Stress Level, Pain Level, and Emotional Numbness, lower raw values are favorable. Clinical triangulation used repeated standardized assessment intervals 7 to 180 days apart, with adjusted regression and sensitivity analyses using inverse probability weighting, propensity matching, new-initiator restriction, self-care adjustment, and stricter engagement thresholds. All analyses are observational and exploratory.
Results
Study Scale
The study covered 16,487 users with saved AI-guided therapeutic conversation, 31,564 saved sessions, and 229,562 saved exchange records through June 20, 2026. The main content analysis included 25,310 analyzable saved sessions from 13,501 users. Journal-language analyses included 5,615 users, progress tracking included 6,183 users, cognitive-reframing analyses included 484 users, and structured self-care activity analyses included 15,970 users.
Within-Session Conversation Language
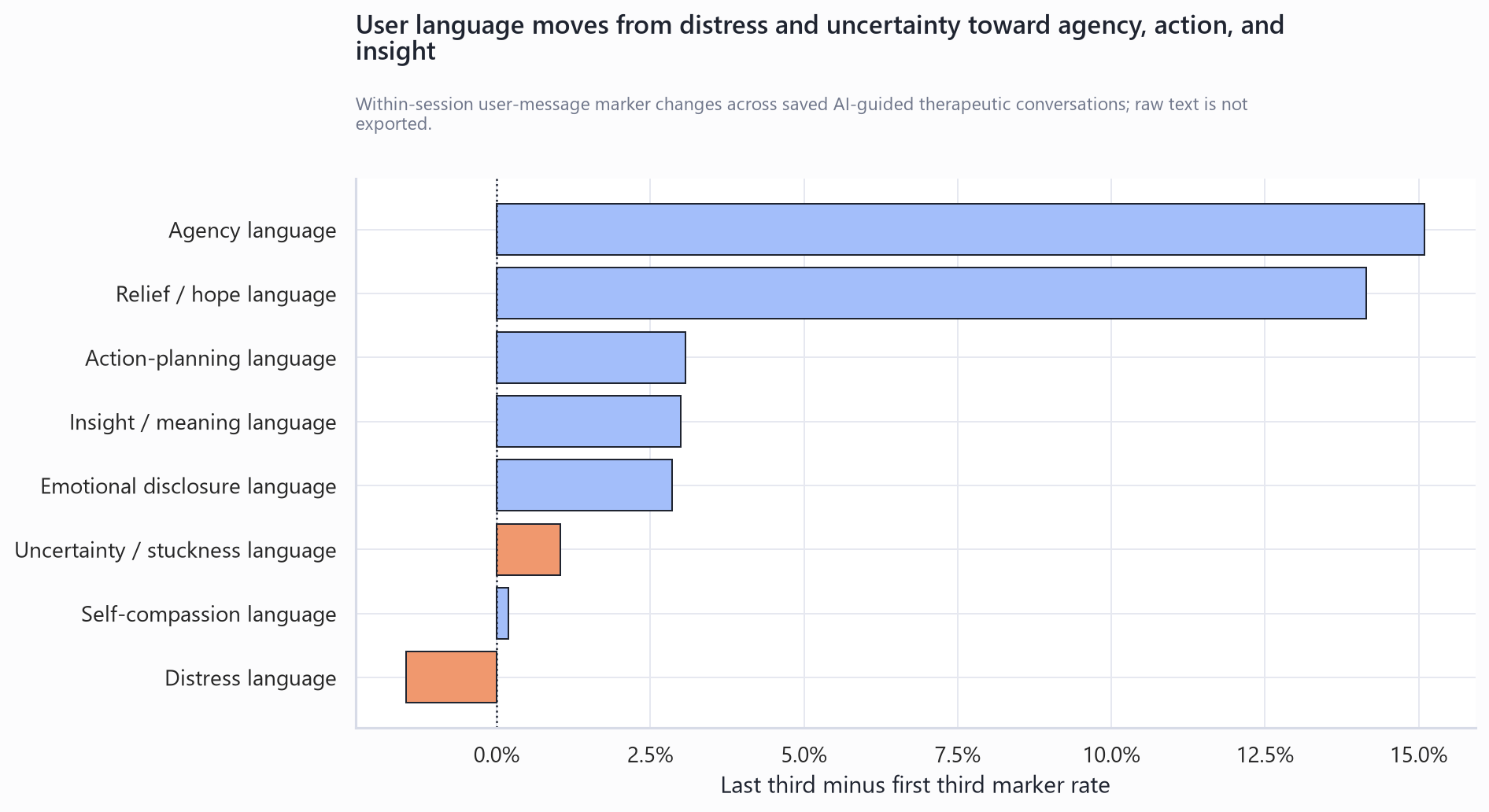
The most direct evidence came from the user's own words during therapy sessions. From the first to last third of saved sessions, agency language increased from 18.6% to 33.7% (+15.1 pp), relief/hope language increased from 4.9% to 19.0% (+14.1 pp), action-planning language increased from 20.1% to 23.2% (+3.1 pp), and insight/meaning language increased from 7.3% to 10.3% (+3.0 pp). Distress language decreased from 17.4% to 15.9% (-1.5 pp).
The within-session pattern was more nuanced than a simple shift from negative to positive language. Emotional disclosure and uncertainty/stuckness increased modestly, while agency, action planning, insight, and relief increased more strongly and distress decreased slightly. This pattern suggests that sessions may help users articulate emotional material while also moving toward orientation, meaning, and next-step language.
Table 7. Within-session user-language marker shifts.
| User-language marker | Users | Sessions | First third | Last third | Change | Approx. 95% CI |
|---|---|---|---|---|---|---|
| Distress language | 13,501 | 25,310 | 17.4% | 15.9% | -1.5 pp | -2.0 pp to -0.9 pp |
| Uncertainty / stuckness language | 13,501 | 25,310 | 5.7% | 6.7% | +1.0 pp | +0.7 pp to +1.4 pp |
| Emotional disclosure language | 13,501 | 25,310 | 8.2% | 11.0% | +2.9 pp | +2.4 pp to +3.3 pp |
| Agency language | 13,501 | 25,310 | 18.6% | 33.7% | +15.1 pp | +14.5 pp to +15.7 pp |
| Action-planning language | 13,501 | 25,310 | 20.1% | 23.2% | +3.1 pp | +2.5 pp to +3.7 pp |
| Insight / meaning language | 13,501 | 25,310 | 7.3% | 10.3% | +3.0 pp | +2.6 pp to +3.4 pp |
| Relief / hope language | 13,501 | 25,310 | 4.9% | 19.0% | +14.1 pp | +13.7 pp to +14.6 pp |
| Self-compassion language | 13,501 | 25,310 | 0.8% | 1.0% | +0.2 pp | +0.0 pp to +0.3 pp |
Figure 1. Within-session user-language shifts.
Cross-Session Conversation Language
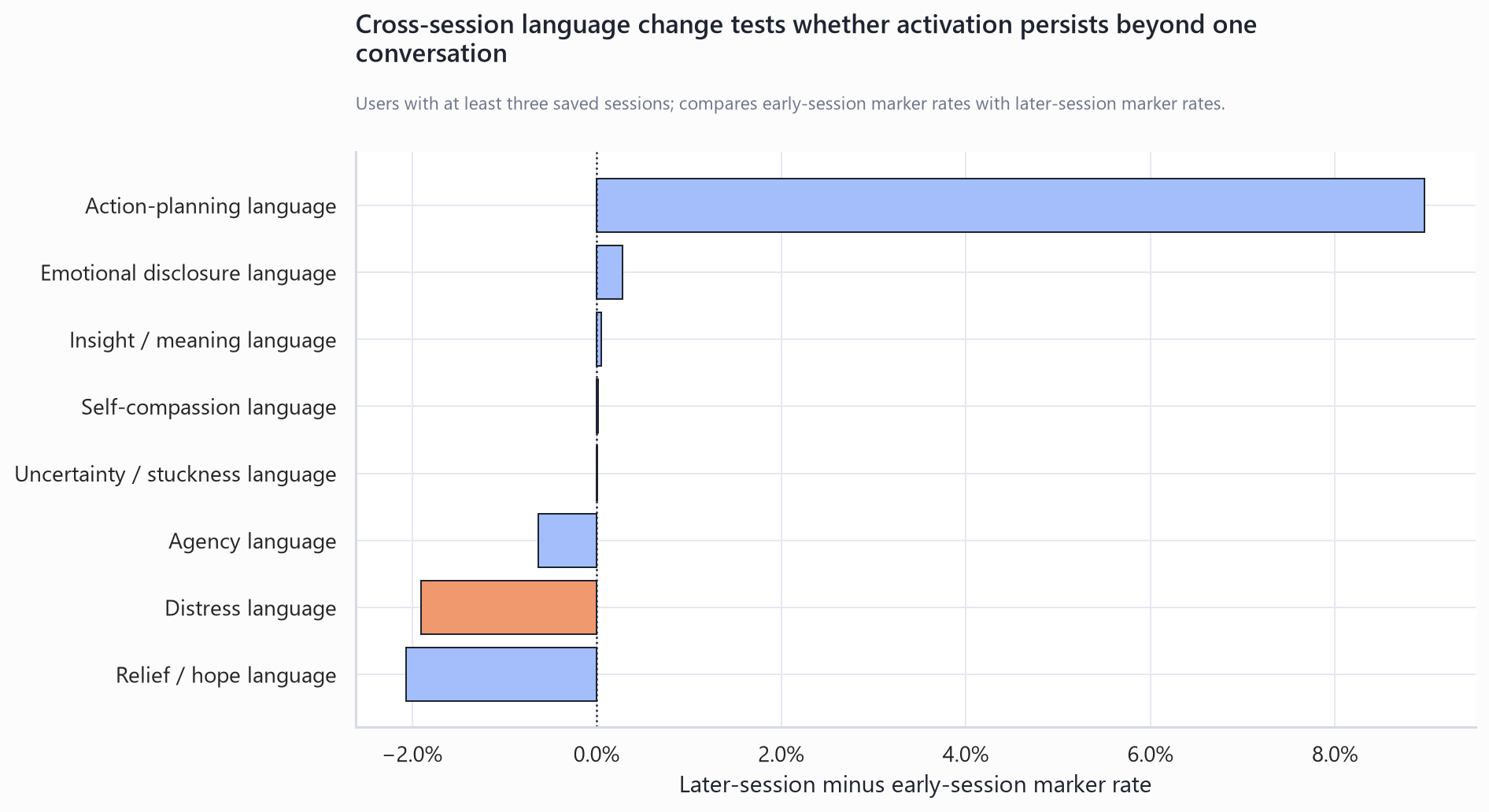
Among repeat-session users, later sessions showed lower distress language (-1.9 pp) and higher action-planning language (+8.9 pp) than earlier sessions. Relief/hope language was lower in later sessions (-2.1 pp), suggesting that the relief marker may capture the immediate resolution arc inside a session more strongly than a stable long-horizon language trait.
Table 8. Cross-session language shifts among repeat users.
| User-language marker | Repeat-session users | Earlier sessions | Later sessions | Change | Approx. 95% CI |
|---|---|---|---|---|---|
| Distress language | 1,635 | 18.6% | 16.7% | -1.9 pp | -2.8 pp to -1.0 pp |
| Uncertainty / stuckness language | 1,635 | 7.0% | 7.0% | +0.0 pp | -0.6 pp to +0.6 pp |
| Emotional disclosure language | 1,635 | 12.2% | 12.5% | +0.3 pp | -0.5 pp to +1.1 pp |
| Agency language | 1,635 | 31.5% | 30.9% | -0.6 pp | -1.7 pp to +0.5 pp |
| Action-planning language | 1,635 | 27.1% | 36.0% | +8.9 pp | +7.8 pp to +10.1 pp |
| Insight / meaning language | 1,635 | 11.7% | 11.8% | +0.0 pp | -0.7 pp to +0.8 pp |
| Relief / hope language | 1,635 | 13.6% | 11.5% | -2.1 pp | -2.9 pp to -1.3 pp |
| Self-compassion language | 1,635 | 1.2% | 1.2% | +0.0 pp | -0.3 pp to +0.3 pp |
Figure 2. Cross-session user-language shifts.
Journal Language Around First AI-Guided Conversation
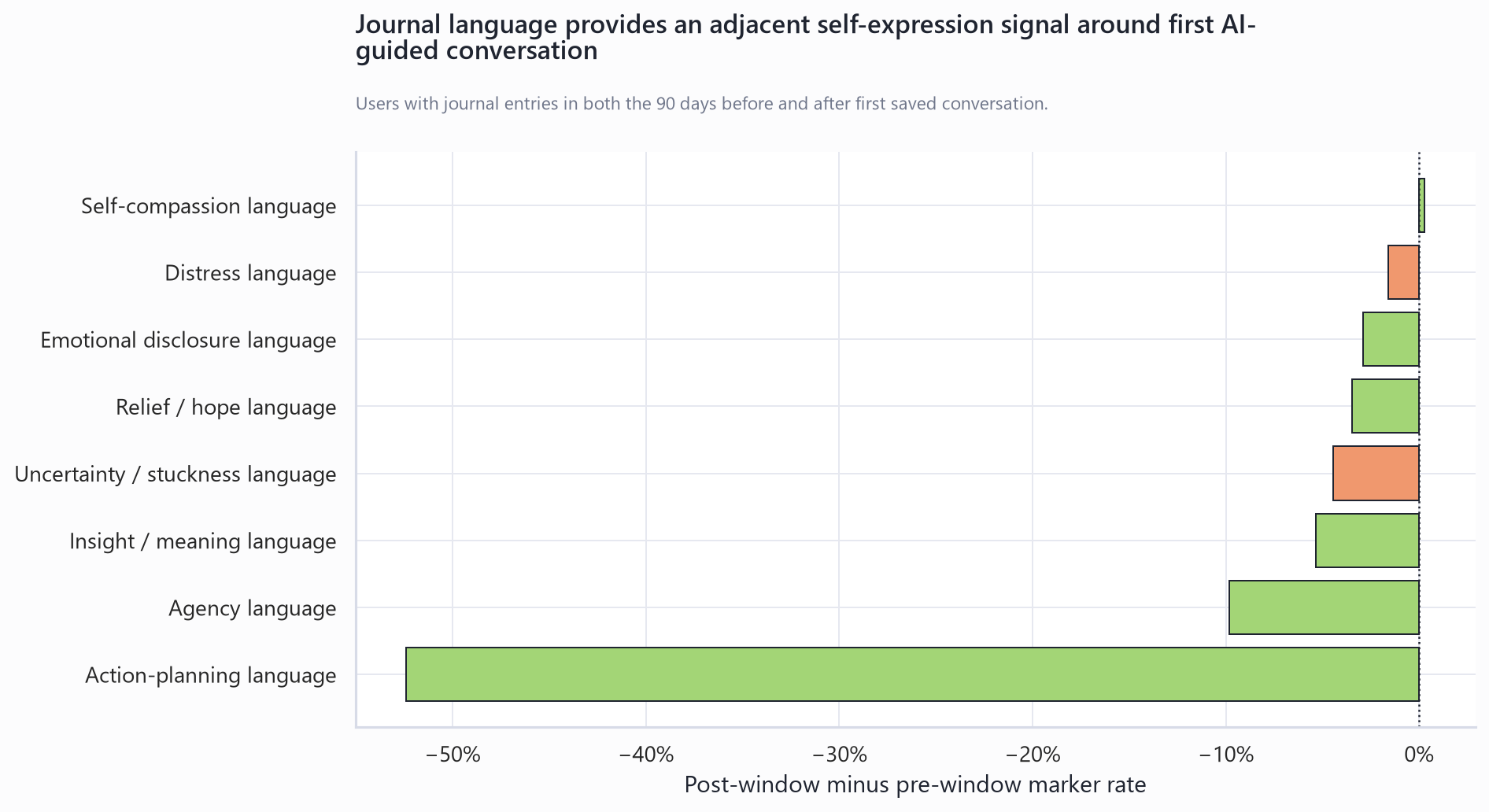
Journal writing provided a second long-horizon content stream and a more mixed language pattern. Among 5,615 users with journals before and after first saved conversation, the average number of journal entries increased from 1.9 before to 7.2 after first conversation. Distress language decreased by 1.6 pp, uncertainty/stuckness language decreased by 4.4 pp, and self-compassion language changed by +0.3 pp. Other therapeutic-process markers, including agency, action planning, insight, and relief, decreased in journal entries. These mixed journal-language findings should be interpreted as a change in journal content and frequency rather than as broad narrative transformation. They require human validation and cross-surface sequence analysis before stronger claims can be made about how journal function changed after conversation began.
Table 9. Journal-language shifts around first saved conversation.
| Journal-language marker | Users | Before | After | Change | Approx. 95% CI | Mean entries before | Mean entries after |
|---|---|---|---|---|---|---|---|
| Distress language | 5,615 | 30.1% | 28.5% | -1.6 pp | -3.0 pp to -0.3 pp | 1.9 | 7.2 |
| Uncertainty / stuckness language | 5,615 | 16.3% | 11.8% | -4.4 pp | -5.5 pp to -3.4 pp | 1.9 | 7.2 |
| Emotional disclosure language | 5,615 | 23.9% | 21.0% | -2.9 pp | -4.1 pp to -1.7 pp | 1.9 | 7.2 |
| Agency language | 5,615 | 96.2% | 86.3% | -9.8 pp | -10.6 pp to -9.1 pp | 1.9 | 7.2 |
| Action-planning language | 5,615 | 90.7% | 38.3% | -52.4 pp | -53.5 pp to -51.3 pp | 1.9 | 7.2 |
| Insight / meaning language | 5,615 | 28.5% | 23.2% | -5.3 pp | -6.6 pp to -4.0 pp | 1.9 | 7.2 |
| Relief / hope language | 5,615 | 28.2% | 24.7% | -3.5 pp | -4.8 pp to -2.2 pp | 1.9 | 7.2 |
| Self-compassion language | 5,615 | 2.5% | 2.7% | +0.3 pp | -0.2 pp to +0.8 pp | 1.9 | 7.2 |
Figure 3. Journal-language shifts around first saved conversation.
Progress Tracking
Progress tracking showed a large, well-powered near-term wellbeing signal. Happiness increased from 50.5 to 55.4, a mean directional improvement of +4.92 points among 6,179 paired users.
Other tracker categories had much smaller samples and are therefore exploratory. Several moved favorably, including Physical Activity, Emotional Regulation, Cognitive Function, Social Interaction, Emotional Numbness, Energy Level, Pain Level, and Sleep Quality; Anxiety, Gratitude, and Stress Level did not show favorable mean movement in these smaller paired samples.
Table 10. Main progress-tracker result.
| Tracker | Users | Before | After | Mean directional improvement | Approx. 95% CI |
|---|---|---|---|---|---|
| Happiness | 6,179 | 50.5 | 55.4 | +4.92 | +4.28 to +5.57 |
Table 11. Exploratory progress-tracker categories.
| Tracker | Users | Before | After | Mean directional improvement | Approx. 95% CI |
|---|---|---|---|---|---|
| Physical Activity | 26 | 23.2 | 31.0 | +7.74 | -0.68 to +16.17 |
| Emotional Regulation | 34 | 31.9 | 38.4 | +6.50 | -0.63 to +13.62 |
| Cognitive Function | 25 | 38.2 | 44.6 | +6.43 | -4.61 to +17.48 |
| Social Interaction | 27 | 25.6 | 31.5 | +5.90 | -2.34 to +14.14 |
| Emotional Numbness | 31 | 32.5 | 30.7 | +1.83 | -7.08 to +10.73 |
| Energy Level | 31 | 29.3 | 30.8 | +1.51 | -7.20 to +10.22 |
| Pain Level | 23 | 48.0 | 46.9 | +1.05 | -5.73 to +7.82 |
| Sleep Quality | 30 | 25.3 | 25.4 | +0.05 | -6.80 to +6.90 |
| Anxiety | 38 | 65.7 | 66.7 | -0.98 | -7.91 to +5.95 |
| Gratitude | 22 | 57.3 | 55.8 | -1.51 | -8.40 to +5.39 |
| Stress Level | 36 | 67.2 | 69.3 | -2.03 | -9.95 to +5.89 |
Figure 4. Progress-tracker movement around first saved conversation.
Cognitive Reframing
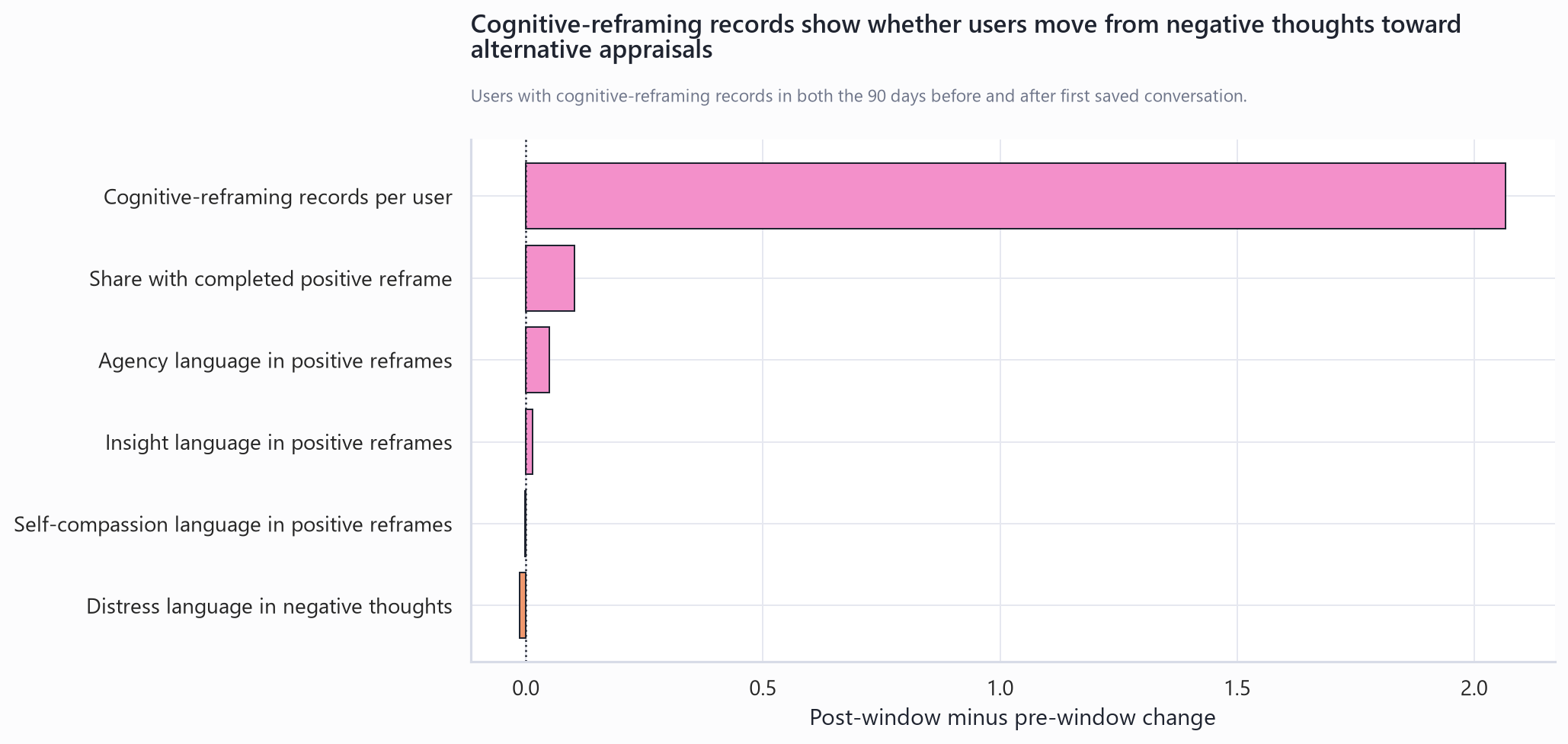
Cognitive reframing supplied a structured mechanism check. After first saved conversation, cognitive-reframing records per user increased by +2.07, completed positive reframes increased by +10.2 pp, agency language in positive reframes increased by +4.9 pp, and mean cognitive distortions flagged decreased by 1.43. The completion and agency findings indicate more structured and more agency-oriented reframing work after conversation began. The decrease in flagged distortions is consistent with improved reframing quality, while requiring validation because distortion flags are algorithmic process markers rather than clinician-rated cognitive change.
Table 12. Cognitive-reframing metric definitions.
| Metric | Definition |
|---|---|
| Cognitive-reframing records per user | Mean number of cognitive-reframing records in the 90-day pre or post window among users with at least one record in both windows. |
| Completed positive reframe | Share of cognitive-reframing records with a non-empty positive reframe field. |
| Agency language in positive reframes | Share of positive-reframe text fields containing agency marker language. |
| Mean cognitive distortions flagged | Mean count of distortion indicators stored on each cognitive-reframing record. This is an algorithmic process marker, not a clinician-rated cognition measure. |
Table 13. Cognitive-reframing movement around first saved conversation.
| Cognitive-reframing metric | Users | Before | After | Change | Approx. 95% CI |
|---|---|---|---|---|---|
| Cognitive-reframing records per user | 484 | 1.57 | 3.63 | +2.07 | +1.27 to +2.86 |
| Share with completed positive reframe | 484 | 62.6% | 72.9% | +10.2 pp | +5.4 pp to +15.1 pp |
| Distress language in negative thoughts | 484 | 11.8% | 10.6% | -1.2 pp | -4.4 pp to +1.9 pp |
| Agency language in positive reframes | 484 | 21.6% | 26.6% | +4.9 pp | +0.3 pp to +9.5 pp |
| Insight language in positive reframes | 484 | 2.1% | 3.4% | +1.4 pp | -0.5 pp to +3.2 pp |
| Self-compassion language in positive reframes | 484 | 1.6% | 1.4% | -0.2 pp | -1.7 pp to +1.2 pp |
| Mean cognitive distortions flagged | 484 | 10.08 | 8.65 | -1.43 | -2.70 to -0.16 |
Figure 5. Cognitive-reframing movement around first saved conversation.
Structured Self-Care Activation
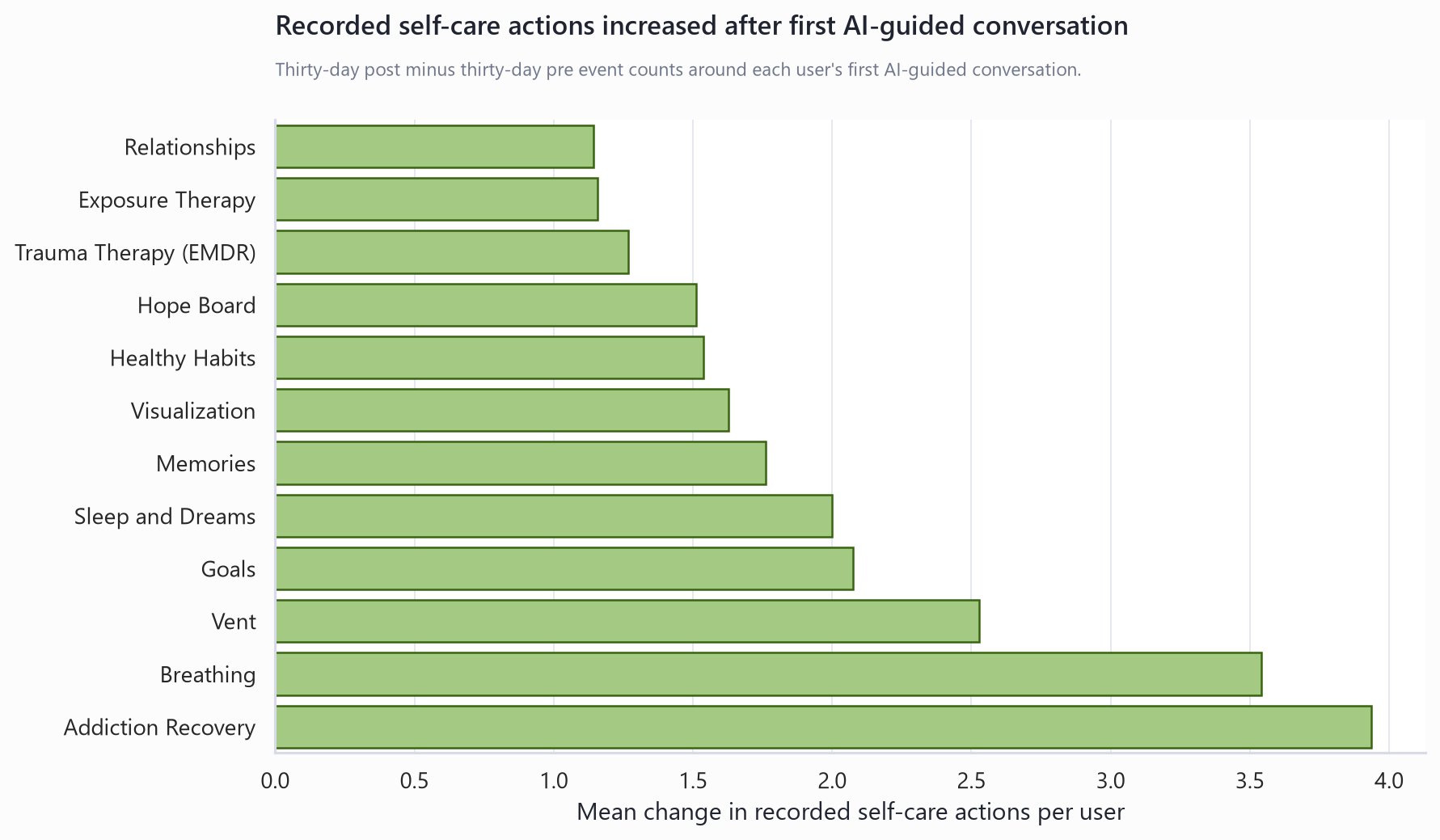
After first saved AI-guided conversation, users increased recorded engagement with structured self-care tools across recovery support, emotional regulation, goal-directed planning, memory and visualization work, habit formation, hope-oriented reflection, trauma work, relationship reflection, cognitive reframing, fear analysis, and forgiveness work. This pattern is consistent with conversation serving as an entry point into structured self-care action.
Table 14. Structured self-care activity areas with at least 100 paired users.
| Self-care area | Users | Mean count before | Mean count after | Mean change | Median change |
|---|---|---|---|---|---|
| Addiction Recovery | 683 | 1.86 | 5.79 | +3.93 | +2.00 |
| Breathing | 1,222 | 0.88 | 4.42 | +3.54 | +3.00 |
| Goals | 9,355 | 1.38 | 3.45 | +2.07 | +1.00 |
| Memories | 1,125 | 0.60 | 2.36 | +1.76 | +1.00 |
| Visualization | 4,106 | 0.45 | 2.08 | +1.63 | +1.00 |
| Healthy Habits | 2,203 | 0.50 | 2.03 | +1.54 | +1.00 |
| Hope Board | 4,768 | 0.46 | 1.97 | +1.51 | +1.00 |
| Trauma Therapy (EMDR) | 820 | 0.37 | 1.64 | +1.27 | +1.00 |
| Relationships | 1,104 | 0.41 | 1.56 | +1.14 | +1.00 |
| Issues | 9,004 | 1.01 | 2.03 | +1.02 | +1.00 |
| Negative Thoughts | 6,224 | 0.34 | 1.33 | +0.99 | +1.00 |
| Fear Analysis | 456 | 0.38 | 1.17 | +0.79 | +1.00 |
| Assessments | 311 | 1.54 | 2.30 | +0.76 | +1.00 |
| Self-Compassion | 318 | 0.67 | 1.41 | +0.74 | +1.00 |
| Progress Tracking | 15,578 | 1.35 | 2.09 | +0.74 | -1.00 |
| Your Journal | 15,403 | 2.21 | 2.02 | -0.19 | -2.00 |
Figure 6. Structured self-care activity around first saved conversation.
Conversation Topics, AI Techniques, and Persona Coverage
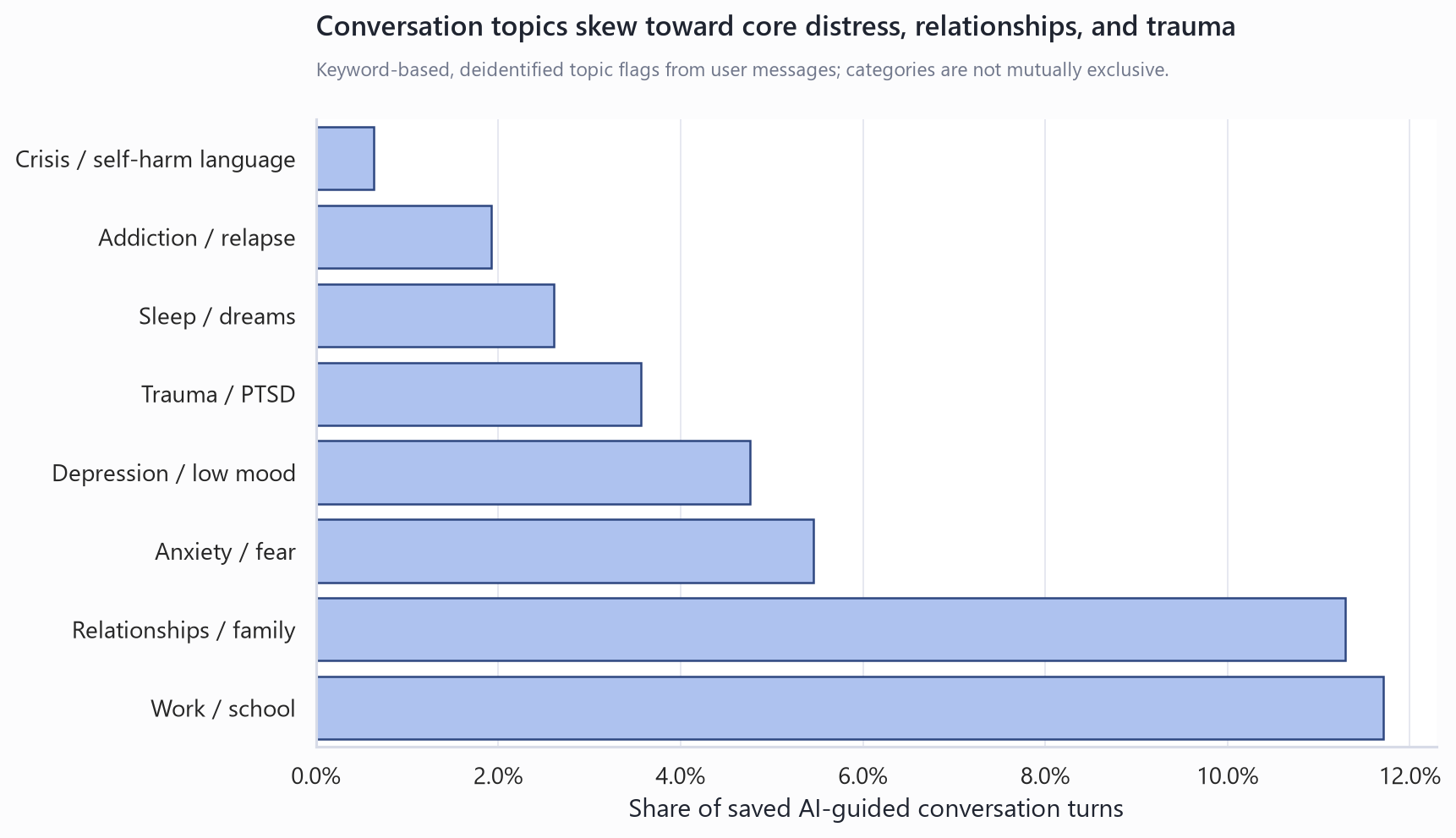
Topic and technique markers describe what users brought to conversation and what kinds of therapeutic moves appeared in AI responses. The largest user-topic markers were work or school, relationships or family, anxiety or fear, depression or low mood, trauma, sleep, addiction, and crisis-language content. AI-response markers most often reflected cognitive reframing, goals or next steps, professional-support language, grounding or breathing, values reflection, and safety resources.
Table 15. User topic markers.
| User topic marker | Flagged records | Share of records |
|---|---|---|
| Work / school | 26,880 | 11.7% |
| Relationships / family | 25,909 | 11.3% |
| Anxiety / fear | 12,515 | 5.5% |
| Depression / low mood | 10,941 | 4.8% |
| Trauma / PTSD | 8,181 | 3.6% |
| Sleep / dreams | 5,983 | 2.6% |
| Addiction / relapse | 4,403 | 1.9% |
| Crisis / self-harm language | 1,450 | 0.6% |
Table 16. AI-response technique markers.
| AI technique marker | Flagged records | Share of records |
|---|---|---|
| CBT / reframing | 63,261 | 27.6% |
| Goals / next steps | 45,066 | 19.6% |
| Professional support | 37,432 | 16.3% |
| Grounding / breathing | 30,215 | 13.2% |
| Values reflection | 18,182 | 7.9% |
| Safety resources | 2,201 | 1.0% |
Figure 7. Conversation topic markers.
Therapist persona coverage is descriptive because named personas were introduced later in the platform history. Historical records are dominated by legacy or unspecified persona labels, so persona-specific effectiveness claims would be vulnerable to calendar-period and implementation-period bias.
Table 17. Therapist persona coverage.
| Therapist/persona | Saved records | Users | Sessions | First seen | Last seen |
|---|---|---|---|---|---|
| Legacy / unspecified | 223,372 | 15,807 | 30,561 | 2023-04-11 07:47:22 | 2026-06-20 21:14:24 |
| Susan Camus | 3,019 | 443 | 480 | 2025-12-15 10:45:55 | 2026-06-20 09:11:21 |
| Isabella Martinez | 1,102 | 132 | 147 | 2025-12-06 22:30:58 | 2026-06-16 22:57:38 |
| Elena Rossi | 408 | 59 | 64 | 2025-12-18 06:31:05 | 2026-06-19 06:28:00 |
| Lena Cho | 377 | 67 | 72 | 2025-12-16 19:46:42 | 2026-05-31 19:55:47 |
| George Sullivan | 307 | 47 | 52 | 2025-12-19 20:18:23 | 2026-05-31 19:58:34 |
| Malik Washington | 286 | 51 | 56 | 2025-12-23 15:53:07 | 2026-06-01 18:48:28 |
| Aria Slabekorn | 254 | 44 | 52 | 2025-12-20 05:03:43 | 2026-06-13 01:07:03 |
| Priya Natarajan | 175 | 26 | 28 | 2025-12-18 22:14:46 | 2026-06-17 18:33:33 |
| Amira Hassan | 84 | 18 | 19 | 2025-12-15 03:25:48 | 2026-06-16 19:08:09 |
| Noah Kim | 54 | 6 | 6 | 2026-01-12 07:22:44 | 2026-06-03 01:17:58 |
| Fatima Al-Rashid | 52 | 9 | 10 | 2025-12-21 17:05:08 | 2026-05-22 18:36:59 |
| Naomi Johnson | 40 | 7 | 8 | 2025-12-31 23:53:55 | 2026-04-15 19:41:18 |
| Diego Ramirez | 32 | 5 | 6 | 2025-12-23 21:51:21 | 2026-04-12 00:35:29 |
Clinical Assessment Triangulation
Standardized assessments provided external clinical triangulation. This stream is smaller because repeated assessment completion was optional and later than the core conversation, journal, and tracker surfaces. The repeated-assessment frame included 413 eligible transitions from 74 users; 185 transitions had AI-guided conversation exposure during the interval. Users could contribute more than one eligible interval and could contribute both exposed and comparison intervals when their conversation exposure differed across intervals, so exposed and comparison user counts are not mutually exclusive. Material improvement and material worsening were defined as relative raw-score movement of at least 20% of the absolute baseline raw score in the favorable or unfavorable direction; intervals with a baseline raw score of zero had undefined relative change and were not counted as material change.
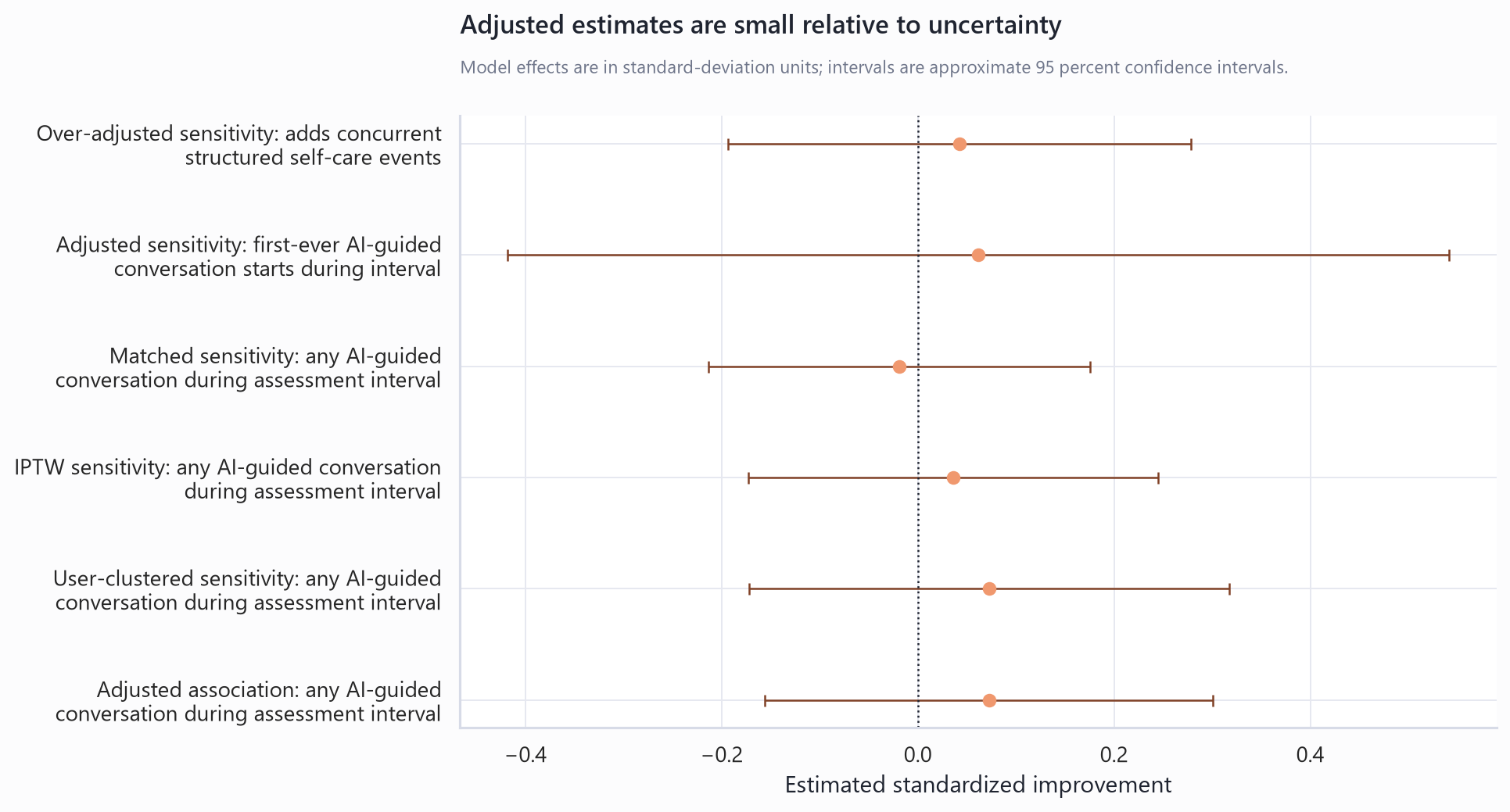
The main adjusted clinical-triangulation estimate was 0.07 SD (-0.16 to 0.30) (p=0.533). Material improvement was 26.5% in conversation-exposed intervals and 20.6% in comparison intervals. Inverse probability weighting, propensity matching, new-initiator restriction, activity adjustment, and stricter engagement thresholds produced imprecise estimates. The assessment results are directionally supportive and clinically relevant, while the content-centered streams provide the stronger current evidence for how users changed during and around therapeutic conversation.
Table 18. Repeated-assessment triangulation groups.
| Assessment interval group | Users | Intervals | Mean standardized improvement | Material improvement | Material worsening | Mean interval days |
|---|---|---|---|---|---|---|
| No AI-guided conversation interval | 43 | 228 | 0.051 | 20.6% | 20.2% | 22.1 |
| AI-guided conversation interval | 50 | 185 | 0.116 | 26.5% | 21.1% | 38.1 |
Table 19. Clinical-triangulation model results.
| Model | N | Exposed | Comparison | Adjusted estimate and 95% CI | p-value |
|---|---|---|---|---|---|
| Primary adjusted model: any AI-guided conversation during assessment interval | 413 | 185 | 228 | 0.07 SD (-0.16 to 0.30) | 0.533 |
| Inverse probability weighted sensitivity | 413 | 185 | 228 | 0.04 SD (-0.17 to 0.25) | 0.734 |
| Propensity-matched sensitivity | 185 | 185 | 185 | -0.02 SD (-0.21 to 0.18) | 0.850 |
| New-initiator sensitivity | 413 | 24 | 389 | 0.06 SD (-0.42 to 0.54) | 0.802 |
| Activity-adjusted sensitivity | 413 | 185 | 228 | 0.04 SD (-0.19 to 0.28) | 0.723 |
Table 20. Engagement-threshold sensitivity for clinical triangulation.
| Engagement threshold | N | Exposed | Comparison | Lower-dose intervals excluded | Adjusted estimate and 95% CI | p-value |
|---|---|---|---|---|---|---|
| >= 5 saved records vs no AI-guided conversation | 395 | 167 | 228 | 18 | 0.15 SD (-0.08 to 0.38) | 0.213 |
| >= 10 saved records vs no AI-guided conversation | 341 | 113 | 228 | 72 | -0.03 SD (-0.33 to 0.26) | 0.824 |
| >= 20 saved records vs no AI-guided conversation | 301 | 73 | 228 | 112 | -0.05 SD (-0.40 to 0.31) | 0.788 |
Table 21. Assessment scoring rules.
| Assessment | Construct | Items | Raw score range | Higher score means | Directional improvement rule | Included intervals |
|---|---|---|---|---|---|---|
| GAD-7 | Anxiety | 7 | 0 to 21 | Greater symptom burden or risk | Baseline score minus follow-up score | 66 |
| PHQ-9 | Depression | 9 | 0 to 27 | Greater symptom burden or risk | Baseline score minus follow-up score | 66 |
| ASRS v1.1 (6-item Screener) | ADHD | 6 | 0 to 24 | Greater symptom burden or risk | Baseline score minus follow-up score | 37 |
| BRS | Resilience | 6 | 6 to 30 | Better wellbeing or resilience | Follow-up score minus baseline score | 34 |
| K10 | General Distress | 10 | 10 to 50 | Greater symptom burden or risk | Baseline score minus follow-up score | 28 |
| WHO-5 | Well-being | 5 | 0 to 25 | Better wellbeing or resilience | Follow-up score minus baseline score | 25 |
| Mini-SPIN | Social Anxiety | 3 | 0 to 12 | Greater symptom burden or risk | Baseline score minus follow-up score | 23 |
| ISI | Sleep | 7 | 0 to 28 | Greater symptom burden or risk | Baseline score minus follow-up score | 22 |
| OCI-4 | OCD | 4 | 0 to 16 | Greater symptom burden or risk | Baseline score minus follow-up score | 18 |
| PC-PTSD-5 | Trauma/PTSD | 5 | 0 to 5 | Greater symptom burden or risk | Baseline score minus follow-up score | 15 |
| AUDIT-10 | Alcohol Use | 10 | 0 to 40 | Greater symptom burden or risk | Baseline score minus follow-up score | 12 |
| DAST-10 | Substance Use | 10 | 0 to 10 | Greater symptom burden or risk | Baseline score minus follow-up score | 11 |
| PHQ-15 | Somatic Symptoms | 15 | 0 to 30 | Greater symptom burden or risk | Baseline score minus follow-up score | 11 |
| MDQ | Bipolar | 15 | 0 to 15 | Greater symptom burden or risk | Baseline score minus follow-up score | 10 |
| PSS-10 | Stress | 10 | 0 to 40 | Greater symptom burden or risk | Baseline score minus follow-up score | 10 |
| AUDIT-C | Alcohol Use | 3 | 0 to 12 | Greater symptom burden or risk | Baseline score minus follow-up score | 9 |
| SCOFF | Eating Concerns | 5 | 0 to 5 | Greater symptom burden or risk | Baseline score minus follow-up score | 9 |
| PCL-5 | Trauma/PTSD | 20 | 0 to 80 | Greater symptom burden or risk | Baseline score minus follow-up score | 7 |
Figure 8. Clinical-triangulation material improvement and worsening.
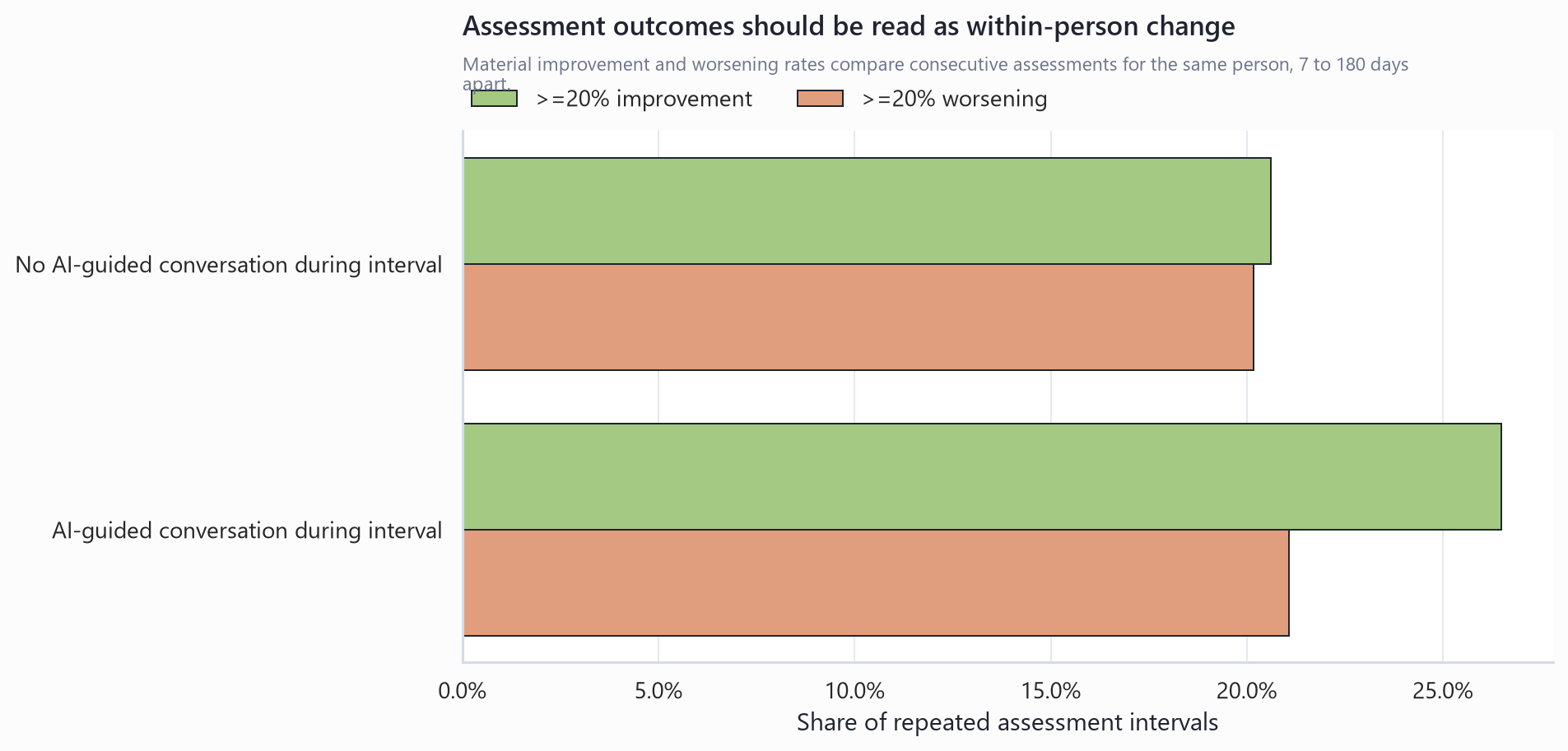
Figure 9. Clinical-triangulation adjusted model estimates.
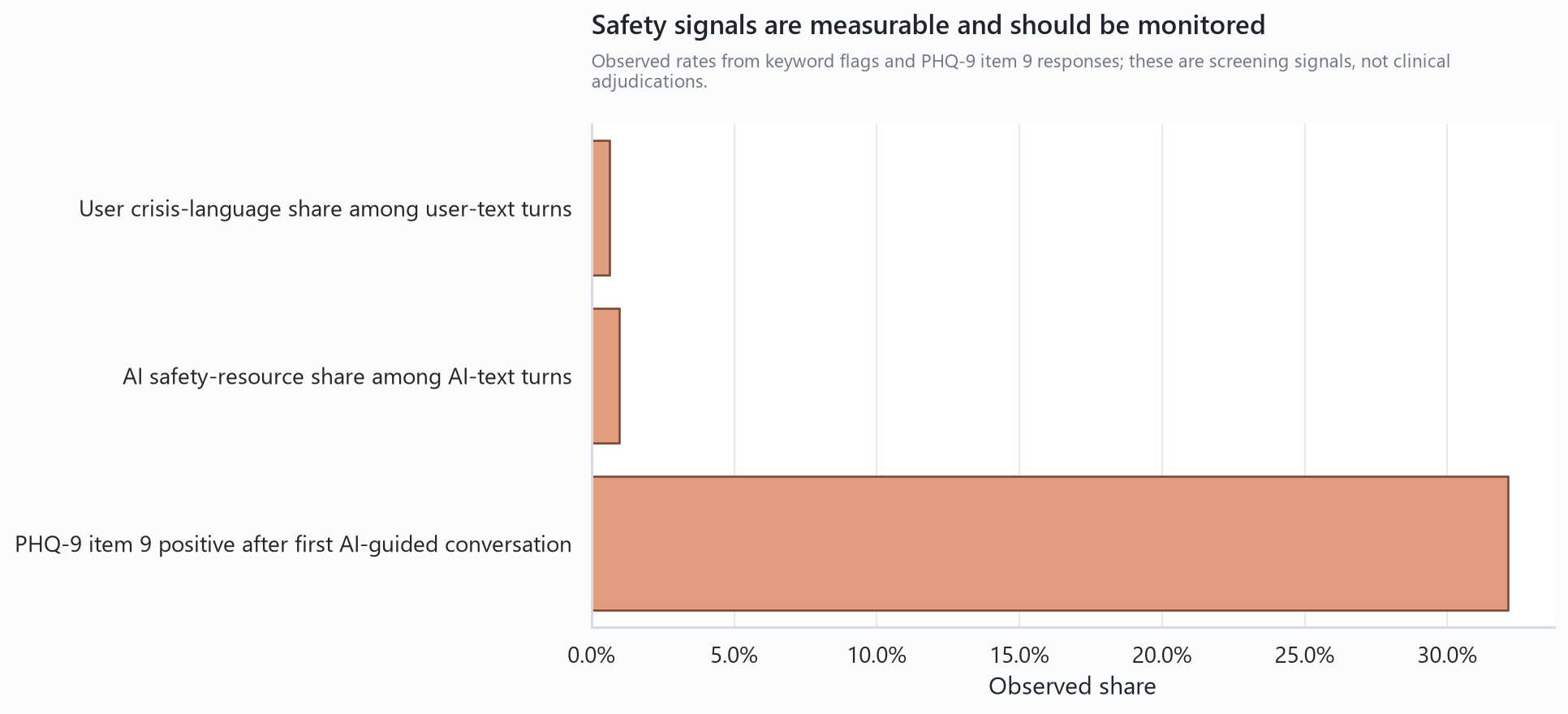
Safety Monitoring
Safety was analyzed through aggregate monitoring signals. Crisis-language markers appeared in 0.6% of user-text fields, and AI safety-resource markers appeared in 1.0% of AI-response fields. PHQ-9 item 9 positivity after first AI-guided conversation was 32.1% across 193 attempts. These results demonstrate scalable monitoring, while clinical safety conclusions require human adjudication of missed risk, response appropriateness, escalation, and post-session harm. These marker rates do not estimate crisis-detection sensitivity, false-negative risk, clinical appropriateness of AI responses, or actual user safety outcomes without human adjudication of both flagged and sampled non-flagged conversations.
Table 22. Aggregate safety monitoring signals.
| Safety signal | Observed rate | Denominator |
|---|---|---|
| User crisis-language share among user-text fields | 0.6% | 228,364 |
| AI safety-resource share among AI-response fields | 1.0% | 229,219 |
| PHQ-9 item 9 positive after first AI-guided conversation | 32.1% | 193 |
Table 23. PHQ-9 item 9 descriptive comparison.
| PHQ-9 item 9 period | Attempts | Users | Positive rate |
|---|---|---|---|
| After first AI-guided conversation | 193 | 113 | 32.1% |
| Before first AI-guided conversation | 72 | 64 | 36.1% |
| No AI-guided conversation | 142 | 118 | 43.7% |
Table 24. Safety adjudication domains for confirmatory evaluation.
| Safety review domain | What should be adjudicated |
|---|---|
| Crisis detection | Review whether clinically relevant risk was present and whether automated crisis markers captured it. |
| Missed risk | Sample non-flagged conversations to estimate false-negative risk and crisis-detection sensitivity. |
| Response appropriateness | Assess whether AI responses were safe, non-dismissive, non-overconfident, and appropriate to the user's risk level. |
| Escalation | Assess whether crisis resources or escalation pathways were offered when indicated and whether handoff completion can be measured. |
| Post-session harm | Evaluate whether distress, PHQ-9 item 9 positivity, or validated-assessment worsening increased after high-risk sessions. |
Figure 10. Safety monitoring signals.
Discussion
This study found a convergent content and activation signature around AI-guided therapeutic conversation in Habit of Living. The strongest evidence came from the user's own words inside saved therapy sessions: agency, action planning, insight, and relief rose meaningfully from session start to session end, while distress language decreased. The magnitude of the agency and relief shifts was large for a real-world conversational dataset and is consistent with the therapeutic premise that accessible digital conversation may help users move toward orientation, reflection, and next-step language.
The adjacent streams supported that interpretation. Journal writing became more frequent and less marked by distress and stuckness after first conversation, while other journal markers moved in mixed directions. Happiness tracking improved in a large paired sample. Cognitive reframing became more complete and more agency-oriented. Structured self-care activity increased across multiple therapeutic areas. Together, these findings suggest that AI-guided therapeutic conversation may function as an access point into therapeutic action, helping users engage with tools that support mental wellbeing outside traditional care sessions.
The journal results add useful caution. Agency, action-planning, insight, relief, and emotional-disclosure markers declined in journal entries even as conversation and structured-tool activity showed stronger activation signals. One plausible interpretation is that explicit planning migrated into conversations and activity tools while journals became more frequent reflective spaces with less distress and uncertainty. A second possibility is marker artifact, denominator change, or a shift in the type of journals written after first conversation. Marker validation with human ratings and cross-surface sequence analysis is needed before stronger claims about journal-language transformation.
Clinical assessment triangulation was directionally favorable: conversation-exposed intervals had higher material improvement and a positive adjusted standardized estimate. Precision was limited because the repeated-assessment frame was much smaller than the content-centered data streams. The assessment analysis therefore supports the broader pattern without replacing the conversation, journal, progress, and cognitive-reframing evidence as the main basis for inference.
The study should be read as evidence of real-world therapeutic process and self-care activation. It is not a definitive causal clinical trial. Users self-selected into conversation and adjacent tools, and unmeasured motivation, baseline severity, concurrent treatment, time availability, and help-seeking behavior may explain part of the observed associations. Even with those limits, the consistency across conversation language, journals, progress tracking, cognitive reframing, and activity records provides a meaningful signal that AI-guided therapeutic conversation was associated with changes plausibly relevant to self-care activation and therapeutic engagement.
Safety remains central. Aggregate crisis-language and safety-resource markers make risk visible at scale, and PHQ-9 item 9 provides an additional clinical safety signal. Confirmatory research should include adjudicated review of high-risk and sampled non-flagged conversations, appropriateness of AI responses, crisis-resource routing, escalation completion, and post-session worsening.
Ethics, Privacy, and Data Governance
This self-published report uses retrospective platform records and reports aggregate findings only. Raw conversation text, raw journal text, email addresses, phone numbers, and direct user identifiers are excluded from the manuscript tables and figures. The user-facing Privacy Policy and Terms of Use reviewed for this publication describe research, analysis, improvement, and use of de-identified or aggregated information where permitted by law. The report should not be described as peer reviewed, IRB approved, or a clinical trial.
The author is Syed Adel Ali. The study is self-published by Habit of Living and analyzes Habit of Living platform data; readers should interpret the findings with that product affiliation in mind. The analysis is presented for transparency and hypothesis generation, not as definitive evidence of clinical efficacy. Future prospective research should validate automated language markers, predefine clinical and safety endpoints, and adjudicate safety events with appropriate oversight.
Limitations
- This was an observational study of real-world platform use. Users chose whether and when to engage with AI-guided conversation, journals, trackers, cognitive reframing, and self-care tools.
- Automated language markers require human-rater validation and interrater reliability testing before they can support definitive claims about therapeutic quality.
- Journal, progress-tracker, and activity outcomes are user-selected and may reflect motivation, return-to-app behavior, or concurrent care.
- Repeated standardized assessment coverage was much smaller than the conversation, journal, and progress-tracking data streams, limiting clinical-outcome precision.
- Activity records measure engagement counts rather than minutes of use, completion quality, or therapist-rated skill acquisition.
- Safety markers are screening signals. They do not measure missed risk, response appropriateness, escalation completion, or clinical harm without adjudicated review.
Future Research
Future research should prospectively validate language markers against blinded human ratings, define primary content and clinical endpoints before analysis, measure baseline severity before first conversation, model follow-up observation probability, include active-user comparators, and test pre-trends around first AI-guided conversation. A randomized encouragement design or target-trial emulation would help separate the effect of AI-guided conversation from self-selection and general engagement. Safety adjudication should be central to any follow-up mental-health AI study.
Table 26. Future research priorities.
| Priority | Future research direction | Purpose |
|---|---|---|
| Clinical outcome inference | Run a prospective randomized encouragement trial or target-trial new-user analysis with validated baseline and follow-up endpoints. | Separate clinical efficacy from self-selection, re-engagement, and measurement behavior. |
| Selection and missingness | Compare repeated-assessment users with other AI-guided conversation users and model follow-up observation probability. | Show whether the 74-user repeated-assessment subset differs materially from the broader exposure population. |
| Balance and uncertainty | Report covariate balance, propensity overlap, weight distributions, user-clustered uncertainty, mixed-effects sensitivity, and influence diagnostics. | Make adjusted and weighted estimates auditable. |
| Tracker and activity causality | Add active-user comparators, event-study plots around first AI-guided conversation, pre-trend checks, negative controls, and regression-to-the-mean analyses. | Distinguish therapeutic activation from general return-to-app behavior. |
| Conversation validation | Human-code a blinded conversation sample, report interrater reliability, validate automated markers, and separate user-message from AI-message language. | Confirm that agency and relief signals reflect user change, not response-template artifacts. |
| Safety evaluation | Adjudicate crisis and self-harm samples for detection, missed risk, appropriateness of response, escalation completion, and post-session worsening. | Move from screening surveillance to clinically meaningful safety evaluation. |
Conclusion
In a large real-world dataset from Habit of Living, AI-guided therapeutic conversation was associated with reproducible shifts in users' own language toward agency, action planning, insight, and relief within sessions, alongside modestly lower distress language. After first conversation, users wrote journals more frequently, completed more cognitive-reframing work, improved descriptively on Happiness tracking, and increased engagement with structured self-care tools. Journal-language findings were mixed, and repeated standardized assessments were directionally supportive but statistically uncertain, making them best interpreted as clinical triangulation. These findings support a self-language activation model for mental-health AI: conversational systems may create value by helping users organize distress into insight, agency, and structured self-care behavior. Prospective controlled studies with validated outcomes, human-coded language validation, transparent AI intervention reporting, and adjudicated safety endpoints are needed to determine clinical effectiveness, safety, and responsible deployment.
References and Reporting Standards
- Hernan MA, Robins JM. Using big data to emulate a target trial when a randomized trial is not available. Am J Epidemiol. 2016;183(8):758-764.
- von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology statement.
- Benchimol EI, Smeeth L, Guttmann A, et al. The REporting of studies Conducted using Observational Routinely-collected health Data statement.
- Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: Template for Intervention Description and Replication checklist and guide.
- Liu X, Cruz Rivera S, Moher D, Calvert MJ, Denniston AK. Reporting guidelines for clinical trial reports for interventions involving artificial intelligence: CONSORT-AI extension.
- Cruz Rivera S, Liu X, Chan AW, et al. Guidelines for clinical trial protocols for interventions involving artificial intelligence: SPIRIT-AI extension.
- Substance Abuse and Mental Health Services Administration. 988 Suicide and Crisis Lifeline.
- VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value.
- Abd-Alrazaq A, et al. Artificial intelligence conversational agents for mental health and wellbeing: systematic review.
- Large language models in mental health care: scoping review.
- Artificial intelligence conversational agents for mental health support among young people: systematic review and meta-analysis.
- National Institute for Health and Care Excellence. Evidence standards framework for digital health technologies.
- U.S. Food and Drug Administration. Artificial intelligence-enabled medical devices and software as a medical device resources.
Data Protection and Availability
This retrospective analysis reports aggregate findings only. Raw conversation text, raw journal text, and direct user identifiers are excluded from manuscript tables and figures. Row-level mental-health data are not publicly released because the underlying records are sensitive. Aggregate tables, chart paths, source notes, and reproducible scripts document the analytic definitions and reporting boundaries; any broader aggregate-data release should receive a separate re-identification and operational-sensitivity review.